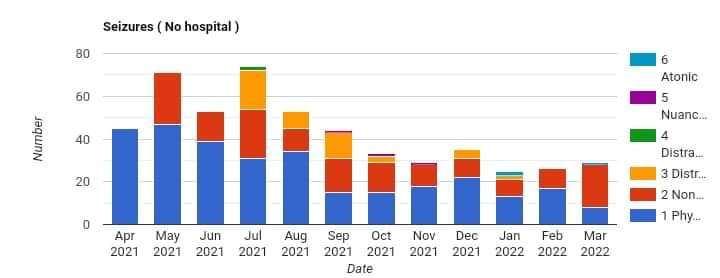
Not a chart I ever imagined I would put together but then again who knows what journeys we all have. This excludes the first few dark days in hospital. Approaching my first anniversary. Update being worked upon.
Not a chart I ever imagined I would put together but then again who knows what journeys we all have. This excludes the first few dark days in hospital. Approaching my first anniversary. Update being worked upon.
An analogy and the 1st April was yesterday



Put yourself into the cramped lunar module. With just minutes left to land, bells start ringing and buttons are flashing, trying to get your rapt attention. Nearly immediately, the astronauts realized they didn’t know what the error code signified, and so they (remarkedly) calmly brought it to the attention of mission control:
“It’s a 1202.”
Within mission control, there were blank stares as by-and-large no one knew what the 1202 was about. Meanwhile, Steve Bales, a guidance officer, called over to a backroom area where various engineers were stationed and ready to dig into any system related matter that might arise.
“1202. What’s that?” he reportedly asked.
John “Jack” Garman, a NASA engineer, took a look at a list he had handmade of the numerous error codes that the teams had come up with.
He realized that the 1202 was a code meaning that the guidance computer on-board the landing craft was getting overloaded with tasks. The programmers had anticipated this overloading might someday occur, and so had established a system internal aspect that would automatically do a fast reboot and then a memory restore to try and get the computer back underway.
Well another milestone comes and goes.
Today I hit the 600 seizures mark. Not even reached the first anniversary yet.
Still okay with it all.
The tiredness and having to allow myself lots of resting time, is draining and reduces your useful hours.
Small price to pay I guess.
Well as I approach the anniversary of my first seizure, it would seem appropriate to review the years data. I shall be doing so in the coming weeks.
A few snippets in advance.
Overall progress. Very pleasing.
Why.
Let us consider the starting point.
Whilst my first seizure sequence required emergency assistance and paramedics, I did not enter what is called status epilepticus. I was in hospital for a short period.
My second sequence, which resulted in a five day hospital stay, was after I had entered into ‘tonic clonic status epilepticus’. It required substantial intravenous medication to stabilise me.
A copious amount of diazepam by two crews of paramedics. So much so, that they ran out. It was not a promising day.
You can google ‘tonic clonic status epilepticus’. Suffice to say it is not a good place to be. I am thankful to the paramedics.
I have had no further sequences which have resulted in medical intervention.
It is only natural to reflect upon one central question. Was there an event which triggered the beginning.
There is no settled opinion within the body of thousands of years of science and reports of people who have had seizures. One common thread though is trauma. In the months prior to my first seizure I had repeated ear infections and burst ear drum which is suggestive of a trauma event to my sensory and hence neural processes.
Since then, I have learnt a great deal and have been able to ‘manage’ my seizure activity. There is no cure. Just management. I have come to know and respect my aura. I have a good appreciation of my trigger events.
I also now experience events which are more akin to tremors but which do not develop into a full physical seizure. This is really the seizures that I now by default ‘distract’ and which are the product of neuroplasticity. It suggests that I have unlearnt the neural pathway which leads to some physical seizures and that this has led to new neural pathways.
I do not consider these events as physical seizures any more for the purpose of reporting. They are a lesser event and are different to the physical seizures which I still have.
What is somewhat reassuring is my model of probability and it continues to show promise.
Whilst I think on, I am neither prescribed nor take specific medication
My seizure activity remains variable. For example, whilst on holiday this month and ‘relaxing’ the ratio of physical to absence seizures reversed. This is the third set of data showing this reversal. The ratio in March is one (1) physical to four (4) absence seizures. REM sleep is also lower in line with the increased absence activity.
The overall probability of me having a seizure is currently sat at 0.9 per day. I do not have seizures EVERY day. When I do have seizures they cluster.
Consider that in the first few days, I was experiencing over twenty (20) seizures a day.
As an aside, this is suggestive as to why so many people have been previously incorrectly diagnosed with epilepsy.
Epilepsy is defined as being at least two seizures without a known trigger (unprovoked seizures) that happen at least 24 hours apart.
This diagnosis has resulted in quite powerful medications being prescribed which have significantly harmed the person having seizures.
It has also masked what is actually happening.
More to follow in the next monthly update.
I remain very positive and we are already making plans for our next breaks in June, September and October. It would seem that a three month cycle works well.
In response to a post on the FND site.
Last night I had a non epileptic attack during an episode of full body paralysis. It’s the first time I’ve experienced both at the same time. I mostly find it curious, from the perspective of someone who studied psychology at uni ten years ago and has an interest in how the brain works. My brain doesn’t want me to move, and wants me to move too much at the same time 😅
My response.
Raises the interesting debate about the interplay of rem sleep moving between the two states of paralysis and non paralysis and the same interplay between consciousness and subconsciousness. The text books say neither can occur at the same time based upon a binary view of only two states. Anything else is called a disorder. Same philosophical debate happened when it was understood waves can behave as particles and thus quantum mechanics was framed. We need now to think of the neural interplays not as binary events but as quantum probabilities. Food for thought.
After a tiring January where the recovery time from my seizures has increased, we have decided to take another holiday.
To break the cycle and to get a little bit more sunshine.
Mid March it is then, we will have another four hour flight. Then some pleasant distracting surroundings.
Looking forward to it.
The most problematic type of my seizures to manage remains my absences.
Why.
Well the whole management philosophy of coping with seizures is to learn to identify, predict, distract and prevent. This is primarily driven by being able to differentiate and recognise the preceding aura.
With absences, you become absent before you have had the chance to interrupt the process of the aura becoming a seizure. You know that you are becoming absent. You know you are absent. You enter a strange state. There, but not present. Your awareness of certain sensations is heightened. For example, I become acutely aware of my breathing which is deeper.
After months of trying to clearly differentiate a specific aura which precedes an absence, I have been able to do so.
As with all my seizures, I experience the general aura of my legs filling up with hot water, as if I were a hot water bottle. This is of course the sensation of plussing. Where the small capillaries fill with more warm fluid. If you will, a flushing sensation or blushing as you can see on some peoples faces.
But what about this specific absence aura.
My eyes. I can now detect small wobbles in my eyes.
Perhaps not noticeable to others. The way I can best describe them is that they seem similar to that which you can observe of someone who is in REM sleep. The rapid eye movement. I exaggerate the description of movement to make the analogy as the wobbles are subtle and not large.
This aura has been consistently felt and has then led to an absence. I can now predict an absence.
Whooppee.
The trick now is to learn how to distract. Work is now in progress on that front.
I have always believed that the best outcome for any condition is to become your own self advocate. Know as much as possible and learn everyday. You can never stop learning.
Below is a snippet from the latest international study concerning FND published in the BMJ yesterday. I have cut and pasted the incidence and prevalence paragraph.
Not that many of us about….but glad to be categorised as young.
Incidence and prevalence of FND
FND is a frequent and disabling condition affecting young people and has a poor prognosis in many patients. The incidence rate of mixed FND is estimated at 4-12/100 000 population per year. Motor FND (abnormal movements and weakness) is estimated at 4-5/100 000 per year, and seizure type FND (also known as psychogenic non-epileptic or dissociative seizures) at 1.5-4.9/100 000 per year. Prevalence studies are scarce, but the reported rate of FND is around 50/100 000 in the population. The prevalence of seizure type FND is estimated at 2-33/100 000
Second mri with contrast of brain and neck. Let us see what this one shows and if there are changes from the one in April 2021, the baseline. It should be reported with 1 to 8 days hence.
First atonic seizure event.
Aka drop seizure. I was standing with a cup of coffee and the lights went out.
Complete loss of consciousness.
No warning, no time to do anything. Did not even feel the floor when I collapsed.
No injuries just coffee everywhere. Soft carpet landing.
Another experience.