March 31st 2023. 719 days after the first seizure event.
Well now. Apologies in advance for the colourful language. The second anniversary of the appearance of the ‘The insidious little bastard’ (my pet name for a functional seizure) approaches and what a difference a year makes.![]()
![]()
At T + 719 days (t=onset) I remain at the magic number of 0, null points, zip – all types of seizure for > 95 days.
- last physical seizure > 395 days ago
- last drop attack > 95 days ago
- last absence seizure > 101 days ago
- last tonic seizure > 144 days ago
vs. 1 year ago…

My good progress continues.
Cautiously optimistic – nature is a fickle creature. Quietly though, very pleased indeed with this.
So I asked Chat GPT what it thought about matters. I think ‘it’ concurs with my world view.
Neuroplasticity refers to the brain’s ability to change and adapt in response to new experiences, learning, and injuries. The brain is not a static organ; rather, it is constantly changing and reorganizing itself throughout our lives.
Neuroplasticity occurs through a process called synaptic plasticity, which refers to the strengthening or weakening of the connections (synapses) between neurons in response to new information or experiences. When we learn something new or experience something novel, our brain creates new neural pathways or strengthens existing ones to better process and retain this information.
Neuroplasticity can also occur in response to injury or disease. When part of the brain is damaged, other areas of the brain can reorganize and take over some of the functions previously performed by the damaged area. This is known as functional reorganization and is why individuals who suffer a stroke or brain injury can often regain some lost function with rehabilitation.
Overall, the concept of neuroplasticity highlights the brain’s remarkable ability to adapt and change throughout our lives, allowing us to learn, grow, and recover from injury.
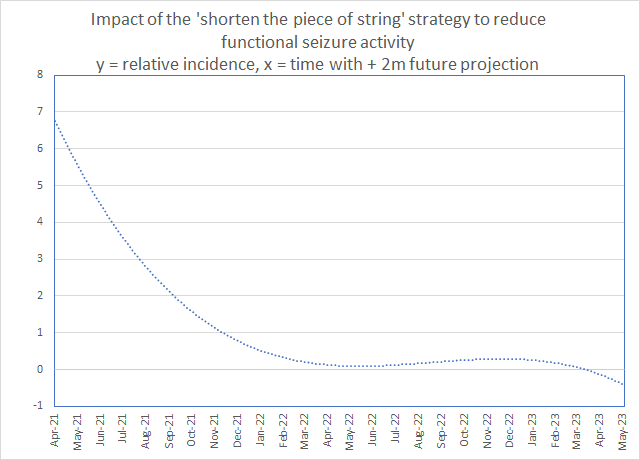
This PR is the ‘likelihood’ of me having a seizure or sequence of seizures in any one given day.
Below is the actual number of seizures over the past 24 months by type showing the reduction.
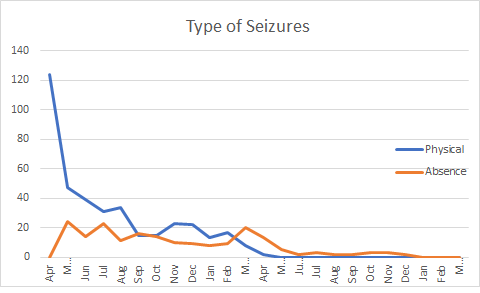
The two diagrams above shows the impact on my seizure activity of me actively using the innate ability of neuroplasticity.
Now for a few musings and they are just that.
I must though once again stress that I make no bold claim or inference as to this being ‘a cure’. It is not. What it shows is the way that I have been able to ‘manage’ my seizures.
As follows, my understanding of my seizures come from the understanding and rationalisation of my experiences. I claim no expertise or ‘specialist’ insight above and beyond any other person who has experienced a functional seizure.
Many will have come across the works of Professor Jon Stone in Edinburgh. He has a colleague and together they have studied and researched the complex facets of functional seizures for over two decades. Professor Jon Stone’s colleagues’ name is Professor Alan Carson and if I may, I shall quote from a tweet of his from last year.
‘Anyone who claims he/she knows everything about the brain is either a fool or a charlatan (usually both).’
I have digressed so let me return to my progress.
For sure, there has been a huge reduction. There is no doubting this. Allied to using this innate ability is the parallel activity of ‘management’. What this means in practice, is that I have identified the triggers which lead to an onset of a functional seizure and mitigated these.
This is not a simple nor a ‘click of the fingers’ activity. It takes considerable time and focus. For me, I was able to identify very soon after onset that my predominant causative trigger was ‘noise’.
I use the word ‘causative’ here in the following context. Let us accept that once you have had a functional seizure, a neural pathway exists. The brain is then primed to enter a ‘functional seizure’ should the ‘causative’ sensation be ‘experienced’ and interpreted by the brain as being the appropriate learnt experience to follow. I do not use the word ‘causative’ in the context of the underlying cause, rather the repetition of a functional seizure event which has the precipitative ‘causative’ sensory ‘fingermark’ of noise.
In the same way that there are many flavours of custard, everyone has a unique ‘fingerprint’ which, at a distance may look similar, but when you investigate the fine print, their uniqueness becomes apparent.
Like many others, it is not just ‘noise’ but a combination of noises which may place you at the tipping point which could lead to a repetition of a functional seizure pathway. I have described this ‘noise’ trigger as being at its highest when in a room where multiple conversations are taking place. I lose the ability to differentiate between conversations and filter, which makes me open on ‘all channels’. The cumulative effect of the noise used to just overwhelm me.
Some, and myself included, describe this as ‘a sensory overload’. As it is a sensory overload, others may experience the same but through other sensations. Common between many is pulsating light and even smells. The common denominator of all of these triggers, is the element that they are of a wave, a frequency or a pulse in character.
I mention this as I have described some sensations which we experience as being both of a particle and wave in character.
Working through this, I discovered that there was a specific frequency which induced my functional seizures. This frequency was 2KHz. I have written about this before.
What is also interesting is that some speakers and in particular those used in hand held devices such as mobile phones hit this sweet spot perfectly. These types of domestic small speakers compress the range of their output to be in the 0.3KHz to 3.4KHz range.
By way of example, for me this means that a mobile phone on speaker phone is an absolute trigger. For many reasons including this, I do not have an ‘Alexa’. For balance, other products are available !
Coming back to the impact of waves, it is worthwhile mentioning that the wave frequency of delta waves is again in the 2KHz range. There has been much written about the frequency of all of our brain waves and what each one means and what they show us.
The science behind this is still emerging and in particular around delta waves. It is thought that delta waves play a much deeper role than previously thought. It is worth remarking upon this deeper role in sleep.
As others have done, I have also described my absences as where you have entered this crossover, this grey area between wakefulness and sleep. They are co-existing during the absence. I have referred to this previously as the ‘cat’ state.
This is beyond the occasional momentary, or for a few seconds, feeling of ‘zoning out’ which everyone experiences irrespective of whether or not they experience functional seizures.
The ‘zoning-out’ feeling to my mind is more of a loss, or a freezing of the attentional aspect of our perception whereas an absence is a much deeper ‘sleep like state’ lasting many minutes and longer. I also liken these ‘zone-outs’ to being auras of a pending functional seizure.
The question I have asked myself on many occasions is the following.
‘Is the environment in which I am in at any given point when I experience a functional seizure, causing the brain to be perturbed in such a way that one particular brain wave is disrupted and/or or entering a state of resonance?’
Maybe a resonance at 2KHz is tricking my own brain to go into this grey area of wakefulness and sleep which I would call an absence.
It is also true that I have put much focus into learning and understanding what the sub-conscious brain is doing by understanding my aura’s. I have then been able to allow my conscious to ‘take control’, to be ‘in control’ or rather to have primacy of decision over my sub-conscious.
This for me was an important lesson to learn as my functional seizures were outside of my control and were involuntary. External stimuli were the trigger not internal emotional ambiguity. Through time though I have been able to exercise a good degree of conscious ‘control’ by learning about their aura’s and retraining the brain so that the pathway which would have led to a functional seizure has now been replaced by a more beneficial pathway.
On this point I must stress here is that functional seizures are involuntary. In no way do I suggest otherwise or diminish this established fact. Rather, I suggest that by understanding that which is happening sub-consciously and to move these processes into our conscious, I have been able to mitigate the functional seizure process by placing ‘control’ within the conscious. A shift from sub-conscious to conscious.
There is also another key aspect which I have used. This is the tracking and understanding of my auras. I have put of lot of energy into this to really understand these as I consider these to be biomarkers.
Others may have a different view as some people do not ‘perceive’ an aura before a functional seizure. Rather the transition from ‘normality’ to ‘functional seizure’ happens without any perceivable warning. I can only imagine the sheer frustration for those who experience this.
I have been fortunate insofar as I have been able to really identify the auras and the sequences which precede a functional seizure event. This sequencing allowed me to work on reducing the functional seizure process to source. To unlearn both consciously and, at an internal biological neural network level, to deemphasise those neural pathways which previously led to a functional seizure. I have tried to explain how I did this in the Process Used document.
What though is the common thread to which all of the above points to, and what is the most impactful activity I have undertaken to reduce my functional seizures.
Timing and the loss of it within the neural network. I have mentioned this before.
What is evident to me, is that the manifestation of my functional seizure is as a result of a loss of timing within the neural network. This loss of timing can be further broken down to be as a consequence of ‘latency’ within the neural network. There is also the dimension of distance. For example, at the start of a physical seizure I noticed this most at the ends of ‘long nerves’ first. In my feet. Allied to distance, is density. Again, at the start of a physical seizure my hands would become tremulous as the first indicator. This relates to the density of nerves in our hands and in particular fingers. Then with absences, all three aspects are compounded in the tightly compact area of our brains. Timing, distance and density.
It is remarkable that irrespective of whether I experienced a physical seizure or an absence seizure, the process I used for interruption was by either rhythmic movements such as duck quacking or by rhythmic noise.
If you will, the use of an external metronome to either interrupt or retrain. This conceptual metronome being a mechanism to alter the timing and questionably the resonance by creating an alternate source of timing to ‘synchronise with’ or resonance.
I touch upon this here, as a full description and narrative of this is a paper in itself. Maybe I should write this.
I am reasonably healthy for my age. My experience of functional seizures seems to have started with multiple severe ear infections leading to mastoiditis leading to seizure activity.
But what about the predisposition. For those who follow and have read about psychology and the talking therapies, there are the infamous P’s. It is worthwhile mentioning here about this model and how it is framed, as it underscores why so many people find psychological interventions to be of little use in relation to functional seizures. The clue is in the second line where it states ‘mental disorders’.
The 4P factor model formulation utilises four types of influences that contribute to the development and progression of mental disorders for a particular patient. These influences are:
- Predisposing risk factors
- Precipitating risk factors
- Perpetuating risk factors
- Protective factors
May I suggest that per se, a functional seizure is not a mental disorder and as soon as people are shown this model they are ‘relegated’, judged’, ‘pigeon holed’ into a flawed model of understanding. Why do I say flawed. It is of a fraudulent Freudian construct. There is no way back from that position once people understand what Freud was suggesting. To balance this, functional seizures do have an impact on peoples lives which may lead to them to be affected in a psychological way. By way of example, if you know that you have functional seizures and let us say drop attacks, these may make you wary of going out and about and doing ‘normal’ activities, as you are fearful of a drop attack. In my mind, this is an effect of a having a functional seizure not the cause.
In defence of talking therapies, if there is one, it is that it can help some people overcome the fear and anxiety which can come about as a consequence of the experience of functional seizures. Again, this does not address the root cause and I personally believe that my progress is due to addressing and mitigating the root causes.
It is worth noting that the proponents of talking therapies openly tell their patients that what they are seeking to do is to address and anxiety and fearfulness as opposed to addressing practical steps of how to reduce the manifestation of a functional seizure. They seek to address the consequences not the source.
You will see throughout my blog the use of a 5th P. This does not relate to predictive as some would suggest as being the natural progression of the 4P’s. This to my mind is again questionable as I describe that the brain does not work within the construct of ‘predictive’ logic. It cannot know about the future in any sense. It works on another P.
That is probability and this is to my mind is the key.
Probability is the likelihood of a past event recurring and what the brain does is store past experiences and draws upon these. For any predisposition the name of the game is to reduce the probability of an event. To be able to reduce functional seizures through probability management.
Now in the same way as in geometry, where there is a magical vanishing point. When you draw two lines to an imaginary infinitely distance spot, the lines converge as if to arrive at point zero, a singularity. However, it can never be arrived at as it is infinite. The laws of probability to do not reduce to zero, the number reduces to an infinitely decreasing level which approaches zero, but never quite gets there.
Once you have had a seizure, the brain is primed, has a learnt response and can and will enter a functional seizure again if allowed to do so.
The tenet of all of my actions I have take in reducing my functional seizures is to reduce their Probability.
As an aside, I read a good book over two decades ago. It is called Nature, Nurture and Psychology published in 1993. ISBN – 1557983968. The debate about Nature vs. Nurture is long in the tooth and the debate upon is a functional seizure ‘organic’ or ‘non-organic’ has been conceptually stuck in the same circuitous argument for much longer. Of course it is both. I use organic and non-organic here not as I believe them but to draw upon the A Tale of Two Turnips which you can find here. It is very well written by Professors Stone and Carson and is far more informative than my clumsy musings.
So enough of the psychology, I can comfortably place that thought process into the metaphorical room 101 bin in this short essay.
From initial infection (the biological trauma) to first seizure was around 3 months. It is worthwhile commenting that I was diagnosed some eight years ago with a REM sleep disorder where the ‘likely’ progression is that within eight years, Parkinson’s is often noted.
When I say likely, it is not a given that one follows the other; it is a statistical observation and as with all statistics, they are only valid at the ‘population’ level and not at the ‘individual’ level. I show no marked signs of Parkinson’s.
I mention this as REM sleep disorders are now thought to be a future marker for some form of movement disorder. This was first studied around a decade ago and is now receiving more interest with emerging studies. I was aware of this potential link after the sleep study which identified the difference in my REM Sleep.
The depletion of dopamine in the latter and an unknown causative event in the former. It is more often than not ideopathic. You are born with it.
So for predisposition one could also say that the fundamental predisposition for my functional seizures was being born. Which is a huge catch all statement, as it suggests that everything is a consequence of being born.
What happens between birth and an event whatever it is, is just experience. That is the nature of life. Life is a collection of experiences. Even though this might sound crass, it is the simple truth. I would refer you to Nature vs. nurture.
Moving swiftly on, I am aware of the use of low level SSRI’s in helping people reduce their functional seizure activity and I shall be jotting down my thoughts on this in light of requests to do so.
I genuinely believe that from day one of the onset of my functional seizures, I have been very fortunate. Within a matter of days I had a ‘solid’, as solid as that which we know about the brain, diagnosis which allowed me to rapidly move through the natural stages of grief, acceptance and to start to put in place a management strategy in the full knowledge that this was going to take a long time and there would be no quick fixes or magic bullets.
I am still learning and as every day and then months pass more of the jigsaw drops into place. What I would say though is this. And it is an open question.
Who are the people who truly understand the functional seizure process and its impact. Is it the people who study the condition or those who experience functional seizures day in day out.
My answer is by way of a thought.
Many years ago, I had occasion to deliver a few talks about neuroplasticity touching upon neurogenesis. During these talks, I purposefully said to all ‘there are no experts in the room’ (which was full of some very serious doctors) and I expanded by saying ‘we are just a group of people who have views and opinions. Some may match and some may differ – there is no definitive answer’.
If I were to address the same audience as I did then, now, I could rephrase the observation. It may be heard as, ‘there are people in the room who have not had a functional seizure and there are people in the room who have had a functional seizure’.
The question to the audience could be, as ‘as an individual non-expert, who would you choose to help you learn about the nature of a functional seizure and its impact.’
Would you choose a person whose font of knowledge comes from a book. Would you choose the observer who watches their friends who do have functional seizures but who do not have functional seizures themselves. Would you choose to learn more about functional seizures and the process from the person who has actually experienced a functional seizure. For context, in choosing you response, take into account that non of the above are experts, and that they will all have differing views based upon the lens of their understanding and context.
It would be an interesting exercise to see as to what the collective vote was.
My preferred vote would be that people should give equivalence to each others views. There are no experts. The views of each group are just as valid and equally invalid. To discount one group, for example those who actually experience functional seizures would not allow you to arrive at a balanced and informed view.
It therefore follows that when forming a view about functional seizures and informing people, you seek the experiences of many people including those who have experienced functional seizures and the context. They can help you to learn about the experience, as each functional seizure is unique, personal and they can explain and describe what it is like.
They ‘get it’.
They are not a inanimate object of, and for, hypothetical conjecture, they are the living, breathing example of that which you wish to understand.
Or to put the question another way, ‘is it exemplary medical practice to be honest and to say I actually don’t know the exact reasons, but let us together work, with open minds, to understand what is going on’. I might then suggest that these are the practitioners who people will trust and who people will seek to find.
Much to think on.
As a further thought, I would like to make a comment about a recent experience I had. Not because I am trying to make a personal point but a much wider butterfly effect observation.
In the past week I had on occasion to help a young lady on the bus I take to my place of work as I have had to surrender my driving licence. That is irrelevant, but explains why I caught this particular bus.
And what followed actually happened.
A nice thing happened today. On the bus a young lady was having an episode of verbal tics and motor tics where she was using her fists to bang her head. She told me she had Tourettes. I explained that I had seizures. I said try this and got her to mimic the duck quacking routine I use to bring my seizures under control. This is just pushing you forefinger onto you thumb rhythmically as if make a quacking duck. Then you ask the person having the seizure to lock on to the rhythm and to copy the actions using their forefinger and thumb. Then to synchronise with the rhythm. She got it and when she was synced her verbal and motor tics and Tourettes stopped as if a switch had been turned off. She was lost for words. Saying ‘this started 15 months ago and no-one has been able to help. This is just so cool’. I suggested she try using it at home with her parents and with her friends. I left her seeing and understanding how a simple rhythmic timing exercise could be used to gain voluntary control again. She was quite taken aback.
I once referred to my onset as being a matter of ‘serendipity’. At the time, some folk queried my use of that word. But you see, through my experience I have been able to help another and this would not have been possible without my own experience.
As some will remember from their days of learning about the nature of ‘energy’, it is never lost. It just transforms from one type to another. In the context of the above, the energy being expended is compassion and this is transferred and passed on from one person to the next. One small action does have a butterfly effect.
Through our collective learning and sharing about our functional seizure experiences we pave the way for further knowledge and understanding. In turn this becomes more widespread. I encourage everyone to learn as much as they can and to share their experiences.
I will finish with the short quotation which I used many months ago setting the scene of my blog. This was and remains:
The capacity to learn is a gift; the ability to learn is a skill; the willingness to learn is a choice – Brian Herbert
I have updated the Seizure Analysis page with the more data but for me these are the key metrics I am using now. This includes a specific example of how REM Sleep can be shown to be a prodrome for my types of absence seizures.
You can see the full data on the Seizure Analysis page. This has data up to and including 31st March 2023.
Thank you for reading my story. I find my functional seizures fascinating and for me they continue to be a great science project for me to get my teeth into. As ever I remain very positive.
To experience is to live, and that is our purpose, whilst we await for our telomeres to finally unravel, and we depart this oasis which sits in the vastness of the universe.