31st October 2022. 568 days after the first seizure event.
Let me begin with some numbers.
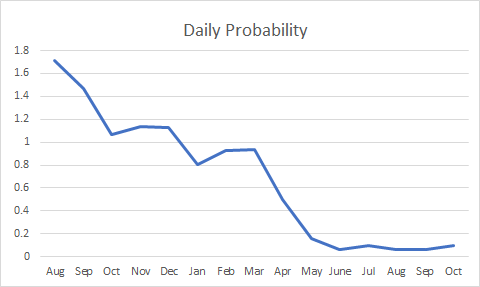
633 total seizures over 537 days and a current probability rate (PR) which has reduced from 6.88 per day on day one to now has been stable at between 0.03 and 0.06 per day for three months.
This PR is the ‘likelihood’ of me having a seizure or sequence of seizures in any one given day.
Below are the two current overall progress charts I use to measure how ‘I am doing’ -the effect and impact of harnessing the innate power of neuroplasticity.
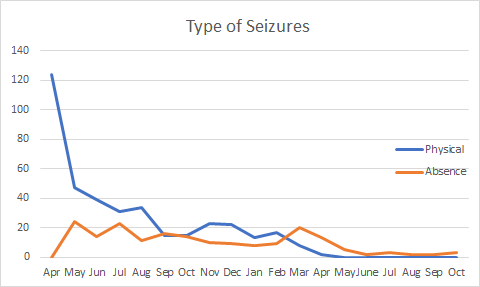
This shows a period of greater than six months of no physical seizure activity coupled with a very low number of absence seizures over the past three months.
This suggests I have ‘stabilised’, ‘plateaued’. I am pleased yet realistic. I say realistic as whilst this shows a current ‘low run rate of seizures’, my predisposition to seizures will probably remain with me. As Lady Gaga sings, in relation to another topic, and I use analogously, ‘I was born this way’.
I am comfortable with that notion.
The eagle eyed amongst you will have spotted an increase in my absences during October. This is true. A 100% increase from two to three.
Is this a trend. Does this show a regression.
The truthful answer is only time will tell.
The comment I will make is I have found that when I have a bacterial and/or ‘virus’ infection, this greatly increases my probability of a seizure. I was consequently not that surprised when I had an absence one day when feeling particularly affected by a respiratory infection which I picked up whilst on holiday. It is reasonable to infer then, that I should be more vigilant with the way I manage my seizure activity in times where I have an infection. No real difference in concept to just generally taking good care of yourself when you know you ‘are not well’. Though with seizures, and having a predisposition, I have to take ‘that little bit extra care’ and maybe curtail certain activities appropriately.
I would like now though to offer a few ‘musings’ if I may. What I would say to the reader is that everyone’s own experience will be unique to themselves. That said, there may be some common threads which others may be able to relate to. I balance that by saying that I make no claim or bold assertion that my experiences represent a ‘generalised‘ view as the experiences I draw upon, and the data I use, are of myself.
When I came home after the initial onset of my seizures, I started to collect data on myself. I have collected information about my seizures since then and now have a dataset of some nineteen months of data. It has allowed me to understand the ‘profile‘ and ‘characteristics‘ of my seizure activity from a variety of angles.
Its primary purpose for me was to help me manage my probability of a seizure event. The clear intent on my behalf was to reduce the probability and therefore the incidence of my different types of seizures by understanding the characteristics of the seizures, and the seizure process. This was evidence based. It is worth noting that, the actual process of data collection had a useful biproduct of ‘objectifying‘ these events and in itself was useful.
At onset, I found that there were no ‘longitudinal‘ studies of outcome and hopefully some of this data may be useful to others in showing the changing profile and nature of my journey.
If I may summarise my own ‘flavour of seizure activity’.
I have experienced two major types of seizures since onset. These I describe as physical – a full-on, whole-body seizure and non-physical – absences. The latter, I found to be more ‘problematic‘ in their management. I joked in November 2021, that I would like to have understood my absence seizures by the time I had experienced a total of eight hundred seizures. Me thinks I may have gone some way towards my ‘target’ after 633 seizures. Understanding more about their cycle, their process and their ‘cute’ sequences and signals. Yes, auras are cute. I have got to know them and their little foibles well over the past nineteen months. Ultimately allowing me to ‘manage my seizures‘ to a level at which I am ‘content’.
I have experienced drop attacks but the number of these has not been in the same order of magnitude as either my physical or absence seizures.
The thinking behind me ‘classifying’ my seizure activity into these two categories was and remains based upon my view that my physical seizures are more of a ‘motor‘ manifestation of the neural disturbance, and my non-physical seizures are more of a ‘temporal’ manifestation of the neural disturbance. It allowed me to work on the physical aspects and separately the temporal aspects. There is no special meaning I attribute here to motor or temporal. It is just how I classify them. I am not trying to rewrite the generally accepted views of others into a ‘new way of thinking’ rather I used this as my ‘internal’ classification to enable me to manage my seizures. After all, my objective was ‘to reduce my seizure activity’
Further, it became apparent to me, that my physical seizures were of two ‘sub-types’. The absences remained as one type and I have not observed any fundamentally different characteristics based upon their time of occurrence.
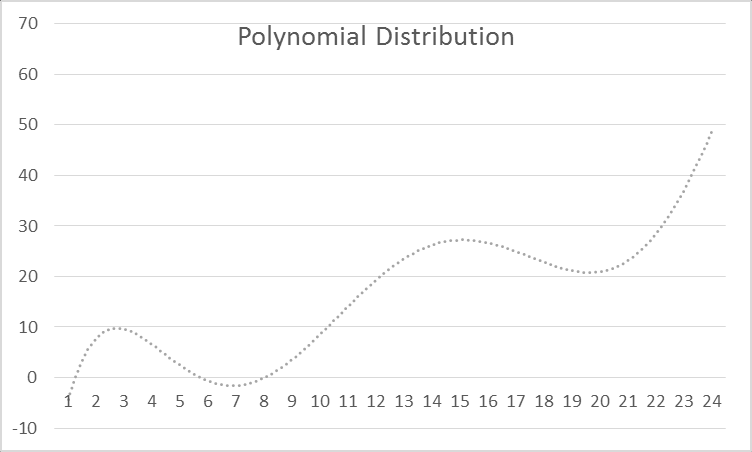
So below are three charts which show the profile of my seizure activity from three of the many angles I view the data upon myself. These different views allowed me to become far more aware of my probability and thus be able to pro-actively interrupt and diminish both my physical and absence seizures.
The first two of these views show what can be described as the ‘circadian’ nature of my seizure activity. The third view shows the correlation between a reduction in REM Sleep as a prodrome preceding absence seizure activity and an increase in REM Sleep post-ictal. This final chart is in itself most intriguing.
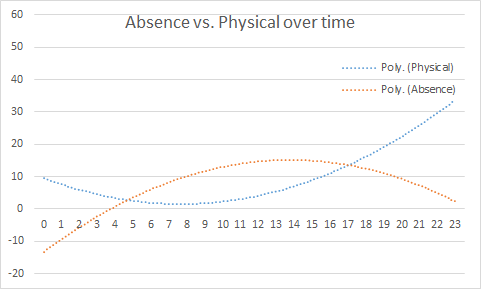
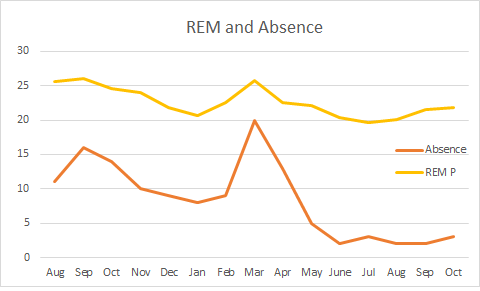
The chart on the left is aggregated into months. When shown as a daily comparator, this shows reduced REM Sleep c. 72 hours prior to absence seizure onset. I would suggest that this is a clear prodrome indicator.
Enjoy and feel free to comment. I am always willing to learn, and I will more than likely publish some other views of the data showing different aspects next month. It is just a function of my available time to do this.
I have updated the Seizure Analysis page with the more data but for me these are the key metrics I am using now. This includes a specific example of how REM Sleep can be shown to be a prodrome for my types of absence seizures.
You can see the full data on the Seizure Analysis page. This has data up to and including 31st October 2022.
Thank you for reading my story. I find my functional seizures fascinating and for me they continue to be a great science project for me to get my teeth into. As ever I remain very positive.
To experience is to live, and that is our purpose, whilst we await for our telomeres to finally unravel, and we depart this oasis which sits in the vastness of the universe.